I think all physicians should have a transparent philosophy about health. Transparency is key to ensure that physicians have skin in the game, and to allow patients or colleagues to address the physician if there are incongruencies between what a physician says and what he does. It is in this spirit that I offer the following philosophical argument: how should a primary care physician think and act? I would venture/posit that over 99% of all practicing physicians don't have a mature philosophy of health. They might be able to recite some position statement from their respective overarching organization, or they might claim (boldly) that they want all their patients to be healthier
and optimize their health
but this term is nebulous, vague, and useless. However, simply because physicians can't put into words what their philosophy of health is, doesn't mean that they don't have one. (Does a child need to have a word for love in order to love their parent?). Most providers innately know what health is, and generally how patients should get there, but that is rarely expressed to others in a way that is easily understood, transparent, and logical. This is my attempt.
I believe that in order for patients to truly be healthy, they must both understand and put into daily practice the concepts of hormesis and of via negativa.
Hormesis is the process by which small doses of harm cause disproportionally large benefits. In modern English, this can be roughly translated into the idiom no pain, no gain.
A healthy life is not always comfortable (in fact, it is frequently uncomfortable), and must incorporate hormesis to take advantage of these disproportionally large health benefits. Practically, hormesis can be found in 3 pillars of a healthy life: exercise, fasting, and vaccination.
Exercise can be thought of as doing slight harm to the body (e.g. via increased heart rate, small muscle tears, buildup of lactic acid; interestingly the exact mechanisms are still largely unknown), which causes a compensatory response of myriad health benefits. (These are almost too many to list here. If you need convincing on the benefits of exercise, I am certainly not the right provider for you.) It is a form of hormesis of which humans have been taking advantage for millennia. There is no exercise or regimen that is one-size-fits-all; find something you enjoy, which is somewhat difficult (i.e. it makes you work hard) and stick to it.
Fasting is another key pillar of hormesis. As I've written, animals that have periodic caloric restriction and consume less calories on average tend to live longer. While this is true only up to a point (it would not be a good idea to go on a 3-week hunger strike), periods of fasting and caloric restriction can improve body composition, inflammatory markers, and longevity. Although the science gets a little complicated (feel free to dive into the literature here), slight harm from the fasting activates cellular and metabolic pathways that are crucial to human health and longevity. Humans weren't meant to ingest a constant IV-drip of calories - there is no law saying you have to eat 3 meals per day, and your metabolism won't slow-down
with fasting to cause weight gain. Being hungry sucks, but it is beneficial in small doses. (For additional information on where/how to start, read this.
Lastly, vaccination is a key exploitation of hormesis. Exposure to very small and relatively harmless parts of disease vectors causes a significant overcompensation by our immune system. When exposure to the actual disease occurs in the future, our immune system is much more easily able to overcome the disease. Vaccination has all but eradicated polio, smallpox, chickenpox (especially in children), measles, mumps, and rubella; it has significantly decreased the incidence of cervical cancer in women, tetanus infections, meningitis, pneumonia, rabies, and yes, even COVID-19. Other than improved sanitation, vaccines are the greatest public health measure of all-time, and should be eagerly obtained if you are serious about your health and longevity.
Via negativa is a very basic and ancient principle that the majority of health benefits can come from eliminating the bad, rather than adding the good. This principle often goes overlooked by patients obsessed with adding the newest dietary supplements or health technology gadget, while simultaneously continuing to overeat, get poor sleep, have high stress, smoke, drink too much alcohol, and/or remain largely sedentary. Eliminating bad habits is arguably much more important than adding new positive habits, and is always necessary (and in many cases is both necessary and sufficient) to achieving optimal health.
Our modern lives are filled with many conveniences that make our lives easier (on paper) but harm our health in the long-run. These negatives should be avoided like the plague; chief among them: the desk-job. It is one of the primary reasons that I have a standing desk, and try not to sit for any longer than 30 minutes (unless I am with a patient).
Additionally, excessive caloric intake (both in terms of the amount of food that people eat, and the frequent timing with which they eat) has never been easier in human history. While it is true that some humans still starve, the USA (and the world to a slightly lesser extent) is a nation of over-consumers: too many calories, too frequently, too convenient. Our biological systems are not meant to have a constant IV drip of food--this has led to the obesity epidemic and increases in many obesity-related conditions: diabetes, cancer, heart disease, etc. Eliminating these excess calories by learning to fast (this is indeed a skill and needs to be learned) is a crucial component of a healthy via negativa lifestyle.
Combining hormesis and via negativa, one gets a powerful combination that is greater than the sum of its parts. The combination of hormesis and via negativa should serve as a lens through which all health decisions are viewed, and it forms the cornerstone of my practice and of my personal philosophy of health. These concepts go far beyond the limited aforementioned examples, and even expand into other domains such as business, finance, and science (although I am no expert in these--my knowledge is largely domain-dependent).
As an example, a patient who periodically fasts (doesn't over-eat) and who exercises and gets vaccinated against communicable diseases is going to be much healthier than a patient who only does one of these things (or certainly a patient who does none of these things).
Let me reiterate: both hormesis and via negativa need to be implemented. Neither is sufficient on its own.
I believe that a primary care physician (or provider; APRNs/PAs can also fill this role) should primarily ensure that patients are adhering to the principles of hormesis and of via negativa. As a sort of "specialist in preventive medicine," primary care physicians are uniquely situated to guide patients towards more beneficial behaviors which, in a perfect world, prevent the patient from getting sick/ill in the first place.
This is a difficult task for several reasons.
First, patients don't listen. They do what they want. It is nearly impossible to be 100% adherent to any recommendation, and as such, patients screw up. It's expected. This inherently makes preventive medicine (and medicine in general) very difficult to apply on a scale that is not 1:1, and therefore all recommendations need to be individualized. This takes time, effort, and money.
Second, it is impossible to quantify preventive medicine. Since we don't live in observable parallel universes, we can never know if an intervention or recommendation prevented a disease or not. Therefore, the only easy thing to quantify is treatment of disease once it has already occurred (i.e. did the patient improve or not?). For similar reasons, since preventive medicine is impossible to quantify, it is impossible to fairly reimburse. No physician can prove that they prevented any disease from occurring. I am rewarded if I treat diabetes; nobody bats an eye if I prevent it from ever occurring. Without good, robust, quantifiable data for preventive medicine, it is nearly impossible to study using traditional statistical methods. Studies tend to be done retrospectively over long time periods, and therefore progress is glacially slow.
Third, the primary care physician is the most dangerous person in healthcare (save for, perhaps, the pediatrician). Let me explain why:
I was recently chatting with a friend who is a surgeon, one who is called when patients end up at the hospital clinging to life from something like an unexpected encounter with a bullet. I told him that I was much more dangerous to patients than he was. He was puzzled. "Not a chance," he said. "If I screw up even one little thing the patient could have incredible complications and lie in a hospital for weeks, or months, with all sorts of infections and lines and medications. If you screw up, someone maybe gets a wrong med and then goes to see a specialist. I'm clearly more dangerous!"
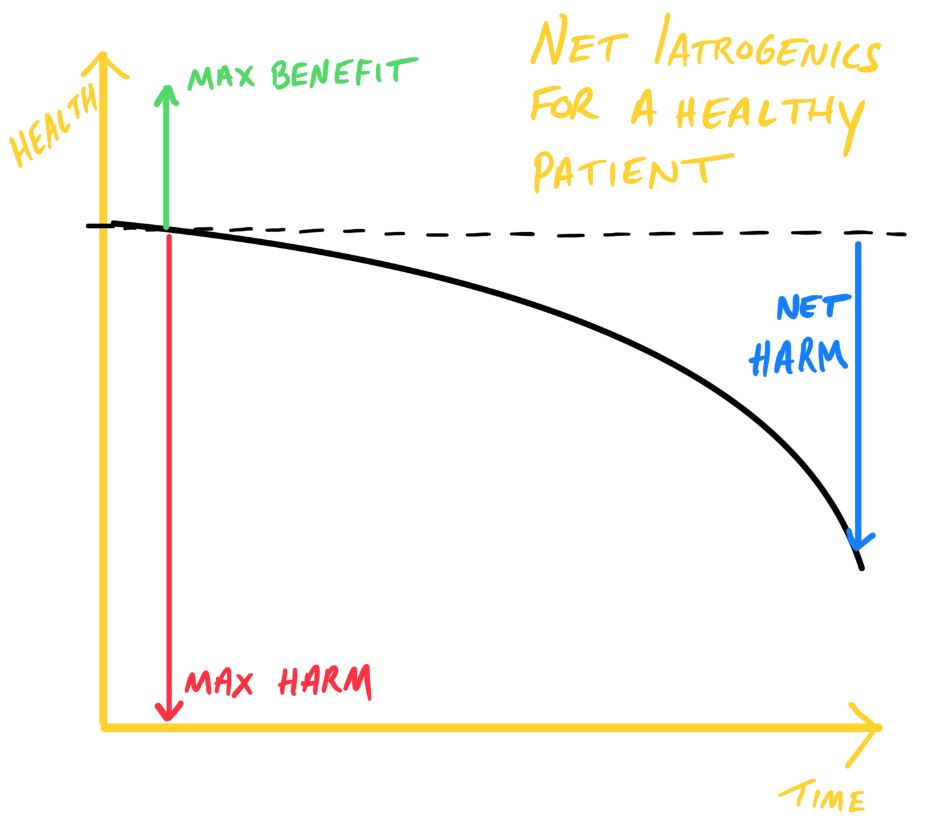
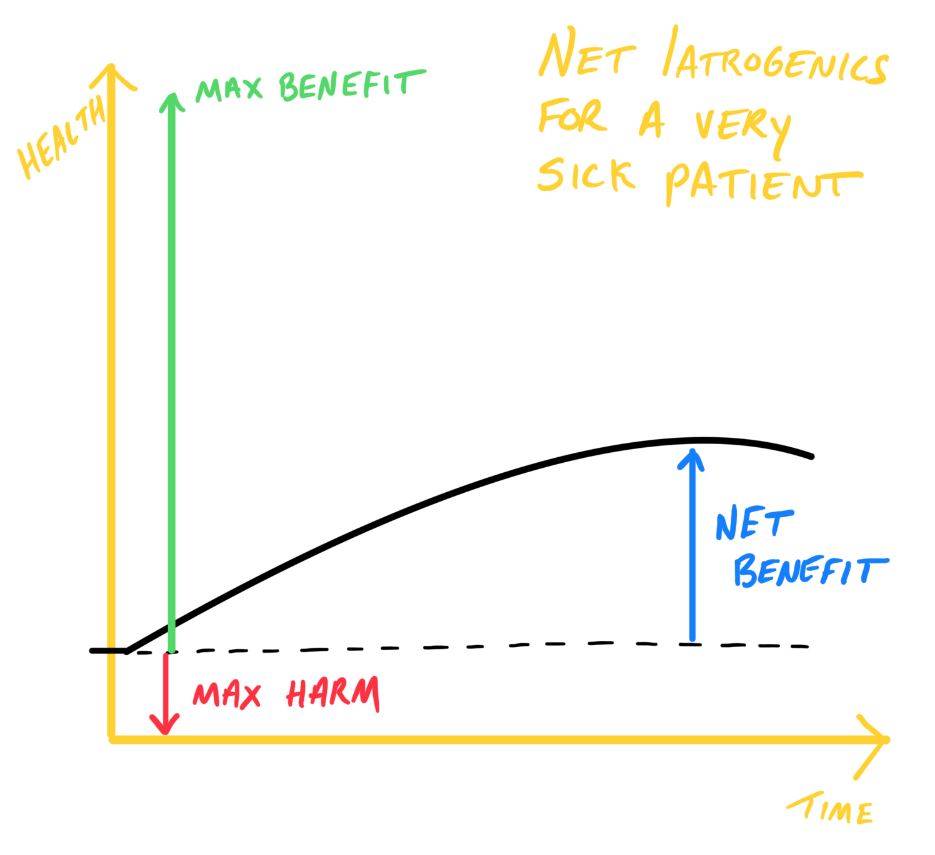
What my friend fails to grasp here is the general principle of iatrogenics. Harm to the patient is a direct function of the patient's starting health, not of the treatment. Since most of my surgeon friend's patients are fairly close to death, intervention will have a net benefit to the patient. You can't cause that much extra harm to someone who is already going to die. You could, however, save his/her life, bringing them back to excellent health. This leads to an overall net benefit to intervention.
The case is the opposite in primary care. A typical patient seeks care when they are already very healthy (such as an annual physical examination) or when they have a relatively minor illness. Any intervention I propose, no matter how seemingly insignificant, could perhaps cause a marginal increase in health, but could also cause a much more drastic decrease in health (i.e. significant illness or death). Therefore, intervention within a healthy patient population is inherently much more dangerous.
Consequently, for healthy patients and minor illnesses, a good primary care doctor will do nothing far more than they do something. This may seem like lazy medicine, but as I've shown above, is actually much better for the sake of the patient (but not necessarily for the wallet of the physician). This form of medicine is very difficult to practice, however. Nobody is rewarded for what they won't or don't do. Actions are rewarded. Interventions are rewarded. Inactivity is often vilified when it should more often be celebrated. This doesn't mean that guidelines should not be followed, or that negligence is something to be championed. It means that a good physician should be savvy enough to avoid intervention for intervention's sake.
A good primary care physician makes it easier for their patients to live by the above principles, and treats patients according to these principles.
However, eliminating naive intervention does not mean that physicians need to reject modernity. In fact, I strongly believe that many modern technological advances have made it easier than ever for patients to engage in hormesis or via negativa. A primary care physician should be knowledgeable about this technology, and how it can be leveraged to help patients. He/she should directly provide opportunity for the patient to trial practical applications of hormesis and of via negativa, such as exercise and fasting. The physician should employ a multidisciplinary team that helps patients with these practical applications, building healthy habits and lifestyles that are sustainable and evidence-informed.
This is something I plan to build.
An excellent physician should also directly practice what they preach. They should never recommend anything to a patient they wouldn't do themselves (or aren't doing themselves), and should be open with patients about what they would do if they were in the patient's shoes.
As examples, patient's shouldn't listen to a physician's weight loss advice if the doc is overweight; shouldn't be counseled on alcohol cessation if the doc drinks too much; shouldn't heed exercise advice if the doc is sedentary; shouldn't be admonished for poor sleep patterns if the doc doesn't get quality sleep; shouldn't adhere to specific dietary advice if the doc isn't adhering to that diet.
Physicians must taste their own medicine. They must have skin in the game. It is perhaps the sine qua nonof the practice of medicine. No risk of harm to others without risk of harm to oneself.
Honestly, I don't really care if patients listen to what I suggest or recommend. My opinion, although given with good intent and with a background of advanced medical training, is not gospel. But certainly I care if they pay attention to what I do.
Primary care physicians can be thought of as the "jack of all trades, master of none." We have to know so much about so much, but we are rarely the expert in any matter. Therefore, we rely on specialists of all sorts to help manage patients and diseases that are a bit out of our scope of practice, or experience, or comfort level.
Increasingly, perhaps due to higher patient volumes, shorter patient appointments, burnout, and/or other factors, primary care physicians are referring patients to specialists long before it is necessary. Indeed, the data show an accelerating pace of placement of referrals to specialists by primary care physicians. Are patients really getting that much more complicated, or are we simply premature in our placement of referrals?
I firmly believe that primary care physicians should manage all conditions to the fullest and best of their ability/comfort level, prior to placing a referral. This seems like common sense, and it is--on paper. In practice, there are time demands, patient demands, and a host of other factors that make it much easier to pass the buck to the specialist and place what I call a lazy referral, which is a referral placed with minimal to no prior workup or thought. I find there to be no good excuse for a lazy referral, and therefore a good primary care physician should only refer when they have exhausted their scope of practice, but having completed a thoughtful workup and/or treatment plan.
Laziness can be a two-way road, however. Specialists often pass the buck to primary care physicians, promising patients "oh your PCP should be able to do that" or "ask your PCP" or something similar to that. When specialists don't follow-up on their own issues or pass them along lazily to the PCP, I call this a lazy punt and I will call out the specialist (typically kindly and always directly and privately to them) for this behavior.
I care about my reputation, but only with certain people. Most of my patients fall into this category, as do my close friends and my family. It is impossible to please everyone, and sometimes by adhering to one's principles, others can be dissatisfied. Indeed, sticking to one's convictions can sometimes make others unhappy. Being decent and kind can help, but in the end you simply can't please everyone.
How should a physician therefore manage his reputation? I think a slight bit of indifference to the opinion of others is healthy, but not too much. In my opinion, the marker for reputational success is the following:
Do patients come back or not? If so, do they recommend their family/friends or do they come back because they don't have any better option? Do you need to advertise your practice?
A truly great primary care office/practice/physician should not need to advertise or market their services, but should grow by word of mouth. Patients should have such a positive experience that they recommend others they care deeply about to have the same experience. If a physician is heavily marketing their practice or services, it must therefore inherently be an inferior practice or service--otherwise people would be clawing at the door to get in due to positive reputational inertia, and marketing would not be necessary.
Take a look at this list of the top 10 businesses that spent the most on advertising in 2019 (to take an example with readily available and reliable data). Are any of them businesses that you'd passionately tell your friends and family about? Are any of them businesses you'd risk your own reputation for?
It should thus come as no surprise that I do not market my practice. I aim to grow the practice by good old-fashioned word of mouth, the most ancient form of reputation management.
If you notice I start marketing my services, run.
Having joy and purpose in daily work as a primary care physician is key to ensuring a stable, robust, and long career. In the spirit of via negativa, the secret to this daily joy is in elimination of as much of the daily shit as possible. (Forgive the curse word, but I think it most aptly and succinctly describes all of the hassle, bore, tedium, and general dissatisfaction that can come with any job.)
First, entitled patients are my bane. I don't care if patients are sick, complicated, uninsured, unsure, ignorant, or grumpy. I do care when patients are entitled, and act as though they are superior to any other patient, or only their concerns matter, or that they are important, repeatedly demand urgent attention for a non-urgent issue, or berate the staff. One entitled patient can ruin the joy in an entire day, and is a quick recipe to burnout of the provider and staff alike. They are a poison to the practice and will be dismissed if behavior does not change. Sick patients don't always have good days, but that's never an excuse to be unkind, impatient, or assume intentional negligence or incompetence.
This begs the question of "what is a primary care emergency?" How does a patient know that their issue is truly non-urgent? Any issue that is not directly related to current, severe symptoms or disease is not a primary care emergency. Lab test results, referrals, medication refills, paperwork, and nearly everything else do not fall into the category of primary care emergencies. The average primary care physician probably gets dozens of messages from patients every day, in addition to the patients they have to see in the office. Trust that your primary care physician is triaging appropriately, and that oftentimes there is someone much sicker in need of direct attention.
Second, heuristics (think of them as "shortcuts") should be used to help decrease the mental energy associated with daily practice, and are accurate more times than not (but not always). I have many (many of which I know internally but do not really have words/sayings for), and here are some of them:
Third, protected personal time is necessary. Despite the glorification of the old-time "personal physician," no physician is, or should be, on the clock 24/7. This is a fast recipe for burnout. It is vital to have time to do things that are necessary (laundry, grocery shopping, sleep) and things that are enjoyable (family time, hobbies, or simply doing nothing at all). The time spent recharging makes the physician better. All work and no play makes Jack a dull boy (and a terrible physician).
Copyright © 2024 JBL IP, LLC